Quick Answer: G6PD deficiency is a genetic condition where the body lacks an enzyme that protects red blood cells from damage. It’s more common in males and often causes no symptoms unless triggered by certain foods (fava beans), medications (some antibiotics, antimalarials), or infections. When triggered, it can cause hemolytic anemia (breakdown of red blood cells), which can occasionally be serious and need urgent care. Most children with G6PD live healthy lives by avoiding known triggers.
Understanding G6PD Deficiency
G6PD (Glucose-6-Phosphate Dehydrogenase) deficiency is one of the most common enzyme deficiencies worldwide, affecting about 400 million people.
What G6PD Does
| Normal Function | When Deficient |
|---|---|
| Protects red blood cells from oxidative damage | Red blood cells break down when stressed |
| Enzyme always present and working | Enzyme is missing or doesn’t work properly |
| Red blood cells live normal lifespan | Red blood cells destroyed when exposed to triggers |
How Common Is It?
| Region | Prevalence |
|---|---|
| Africa | 5-25% of population |
| Middle East | 5-20% of population |
| Mediterranean | 5-15% of population |
| Southeast Asia | 3-15% of population |
| India | 5-15% in some regions |
Causes and Genetics
How G6PD Is Inherited
G6PD deficiency is X-linked (carried on the X chromosome):
| Gender | Genetics | Severity |
|---|---|---|
| Males | One affected X chromosome | Usually more severely affected |
| Females (carrier) | One affected, one normal X | Usually mild or no symptoms |
| Females (both affected) | Both X chromosomes affected | Can be as severe as males (rare) |
Why It Exists
Interestingly, G6PD deficiency may have an evolutionary advantage:
- Provides some protection against malaria
- More common in malaria-endemic regions
- A trade-off - protection from malaria but vulnerability to other triggers
Symptoms of G6PD Crisis (Hemolytic Episode)
What Happens During a Crisis
When someone with G6PD is exposed to a trigger:
| Timeline | What Happens |
|---|---|
| Hours to days after trigger | Red blood cells start breaking down |
| 1-3 days | Symptoms appear |
| 7-10 days | Usually resolves as new cells are made |
Signs to Watch For
| Symptom | What It Looks Like |
|---|---|
| Jaundice | Yellow skin and eyes |
| Dark urine | Tea or cola colored |
| Pale skin | Unusual pallor |
| Fatigue | Extreme tiredness |
| Rapid breathing | Short of breath |
| Rapid heartbeat | Heart racing |
| Abdominal pain | Especially in children |
| Enlarged spleen | May be felt by doctor |
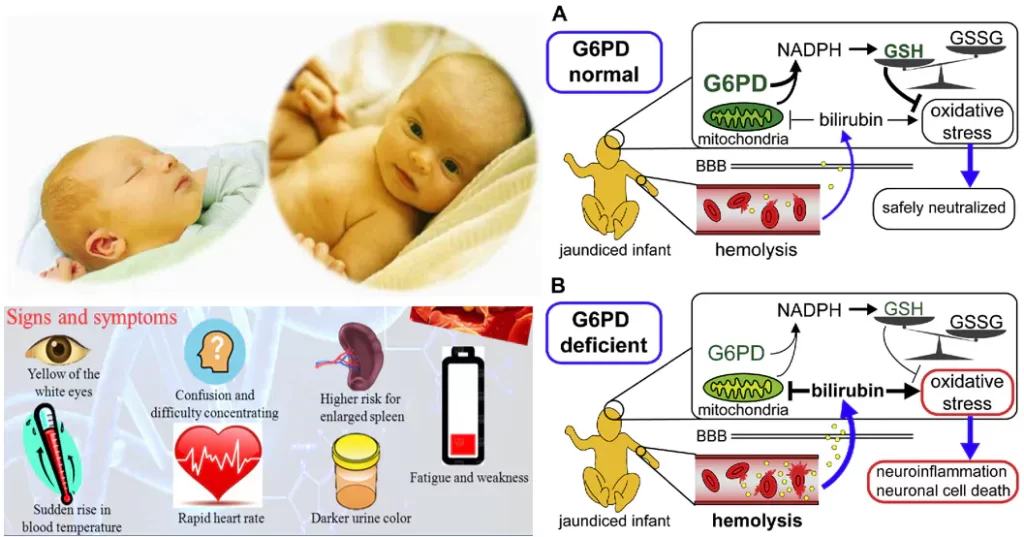
Neonatal Jaundice
Babies with G6PD may have:
- Severe newborn jaundice
- Jaundice appearing earlier than typical (within 24 hours)
- Higher bilirubin levels
- May need phototherapy or exchange transfusion
🚨 Emergency: Any jaundice in the first 24 hours of life, deep yellow colour, a baby who is very sleepy/feeding poorly, or jaundice that is worsening needs same-day medical review. For any baby under 3 months, a fever of 100.4°F (38°C) or higher is an emergency — go to the nearest hospital. In an emergency, call 112 (national emergency) or 108 (ambulance), or go straight to the nearest hospital.
Triggers to Avoid
Foods
| Food | Risk Level |
|---|---|
| Fava beans (broad beans) | HIGH - major trigger |
| Legumes | Some people react |
| Tonic water | Contains quinine |
| Some herbal remedies | Variable |
Note: Fava beans are the most common food trigger. Also called broad beans, bakla, or field beans.
Medications to Avoid
| Category | Specific Drugs |
|---|---|
| Antimalarials | Primaquine, chloroquine |
| Antibiotics | Sulfonamides (Bactrim), nitrofurantoin, quinolones |
| Pain relievers | Aspirin (high doses), phenacetin |
| Other | Naphthalene (mothballs), methylene blue, dapsone |
Always tell doctors your child has G6PD before any medication is prescribed.
Infections
Infections are the most common trigger:
- Bacterial infections
- Viral infections
- Hepatitis
- Pneumonia
- Typhoid
Treatment
During a Hemolytic Episode
| Severity | Treatment |
|---|---|
| Mild | Stop trigger, supportive care, monitor |
| Moderate | Hospitalization, IV fluids, monitoring |
| Severe | Blood transfusion, intensive care |
Long-Term Management
There is no cure for G6PD deficiency. Management focuses on:
- Avoiding triggers (primary strategy)
- Carrying a medical alert card
- Informing all healthcare providers
- Genetic counseling for families
Living with G6PD Deficiency
For Parents of Children with G6PD
| Action | Details |
|---|---|
| Medical alert | Card, bracelet, or necklace |
| Medication list | Keep list of drugs to avoid |
| Inform caregivers | School, daycare, babysitters |
| Read labels | Check medications before giving |
| Avoid fava beans | Even in processed foods |
| Regular checkups | Monitor overall health |
What Children Can Do
| Normal Activities | With Precaution |
|---|---|
| School | Inform school nurse |
| Sports | Usually no restrictions |
| Diet | Avoid fava beans; otherwise a regular balanced diet |
| Travel | Carry documentation, avoid malaria drugs |
Diet Guidelines
| Foods Generally Suitable | Avoid |
|---|---|
| Most vegetables | Fava beans (broad beans / bakla) |
| Fruits | Tonic water (contains quinine) |
| Grains like ragi, suji, rice, dal | Unknown herbal supplements |
| Khichdi, curd-rice | Naphthalene-exposed foods (stored with mothballs) |
| Curd and dairy | — |
Diagnosis
How G6PD Is Detected
| Test | What It Shows |
|---|---|
| G6PD enzyme level | Measures enzyme activity |
| Blood smear | During crisis, shows damaged cells |
| Reticulocyte count | High during/after crisis |
| Bilirubin levels | Elevated during crisis |
When to Test
- Newborn screening (in some countries/states)
- Family history of G6PD
- Unexplained jaundice in newborn
- Anemia after certain medications
- Episode of dark urine and jaundice
Frequently Asked Questions
Q: Will my child outgrow G6PD deficiency?
A: No, G6PD deficiency is a lifelong genetic condition. However, most people with G6PD live healthy, active lives by avoiding triggers. Many go years without any symptoms.
Q: Can my child with G6PD eat at restaurants?
A: Yes, with caution. Avoid dishes that might contain fava beans. In Mediterranean or Middle Eastern restaurants, ask specifically about broad beans/fava beans in dishes.
Q: Is G6PD deficiency dangerous?
A: G6PD is usually well controlled when managed properly. The main risk comes from severe hemolytic episodes, which can largely be prevented by avoiding triggers. A severe episode can occasionally be serious and need urgent hospital care, so know the warning signs (deepening jaundice, dark urine, marked pallor, breathlessness). With awareness, most children with G6PD lead healthy, active lives.
Q: Can children with G6PD receive vaccinations?
A: Yes! Routine childhood vaccinations are safe and recommended for children with G6PD. The vaccines don’t trigger hemolysis.
Q: Should I avoid menthol and camphor products?
A: Yes — be cautious. Naphthalene (mothballs) is a known trigger and should be kept well away from your child’s clothes and bedding. Camphor and menthol products (including vapour rubs) are best avoided in babies and young children with G6PD and should never be applied near the nose or used on infants without your pediatrician’s advice. Check with your doctor before using any such product.
Key Takeaways
- G6PD is manageable - Most people live healthy, active lives
- Avoid triggers - This is the main treatment
- Fava beans are the main food trigger - Read labels carefully
- Always inform doctors - Before any medication
- Carry medical ID - Alert card or bracelet
- Infections can trigger episodes - Seek prompt treatment
- Know the symptoms - Jaundice, dark urine, fatigue
- Boys are more commonly affected - X-linked inheritance
This article was reviewed by pediatricians at Babynama. Last updated: January 2026
Need personalized guidance? Book a consultation with our pediatricians or explore our Care Plans for 24/7 expert support!
Related Tools
This article is for general information for parents in India and does not replace a consultation with your pediatrician. G6PD management, including which medicines to avoid, should be guided by your treating doctor. Vaccinations should follow the IAP (Indian Academy of Pediatrics) immunization schedule. In an emergency, call 112 (national emergency) or 108 (ambulance), or go to your nearest hospital.