The Definitive Indian Vaccination Guide for Children (IAP 2025)
Quick Answer
The Indian Academy of Pediatrics (IAP) 2025 vaccination schedule covers children from birth through 16 years. India’s Universal Immunization Programme (UIP) provides vaccines free at government health centres — BCG, OPV, Hepatitis B, DPT, Hib (as Pentavalent), IPV, PCV, Rotavirus, Measles-Rubella (MR), and Td. PCV and Rotavirus have now been rolled out to all states under UIP. Additional vaccines like Varicella, Hepatitis A, Typhoid Conjugate (TCV), MMR (the mumps-containing version), and HPV are recommended by IAP but available mainly at private clinics, typically costing about ₹500–₹3,500 per dose (figures approximate, vary by city and brand). Vaccinating on schedule is the single most effective thing you can do to protect your child from serious, preventable diseases. Missing vaccines leaves gaps in your child’s protection — but it’s never too late to catch up.
Why Vaccines Matter
Every year, globally, vaccines prevent 3.5–5 million deaths. In India specifically, the impact has been dramatic and measurable.
What India Has Eliminated and Controlled
Polio: India was declared polio-free by the WHO in March 2014 — a historic achievement. Wild poliovirus caused paralysis in hundreds of thousands of Indian children annually through the 1980s and 90s. The Pulse Polio campaign, one of the largest public health drives in history, reached every child under five. We have not had a single case of wild poliovirus in India since January 2011. This happened because of vaccines, and only because of vaccines.
Smallpox: Eradicated globally in 1980. The last case in India was in 1975. A disease that killed 300 million people in the 20th century alone no longer exists — entirely due to vaccination.
Neonatal Tetanus: Deaths from neonatal tetanus dropped by over 95% in India between 1990 and 2015 through maternal Td vaccination and clean delivery practices.
Measles: Cases have dropped dramatically, though India still sees outbreaks in under-vaccinated communities — a warning about what happens when coverage slips.
Herd Immunity: Why Your Child’s Vaccination Protects Other Children
Herd immunity is not a political concept — it is simple epidemiology. When enough people in a community are immune to a disease (through vaccination), the pathogen cannot spread efficiently and outbreaks are suppressed. This protects people who cannot be vaccinated: newborns too young for certain vaccines, children undergoing chemotherapy, infants with immune deficiencies.
The coverage threshold varies by disease. For measles — one of the most contagious diseases known — herd immunity requires about 95% of the population to be vaccinated. When coverage drops below this, measles returns. This happened in Europe in 2018–2019 when misinformation drove vaccine hesitancy and over 80,000 measles cases were reported. India saw a measles resurgence in 2022–2023 in districts with low MMR coverage.
When you vaccinate your child, you are not just protecting them. You are protecting the immunocompromised child in your colony, the newborn next door, the elderly grandparent.
The Cost of Not Vaccinating
Unvaccinated children face real, serious risks:
- Whooping cough (pertussis): Can be fatal in infants under 6 months. 100-day illness with violent coughing fits.
- Hib meningitis: Bacterial meningitis that can cause permanent deafness, brain damage, or death.
- Measles: Still kills children in India, and causes encephalitis in 1 in 1,000 cases.
- Rotavirus diarrhoea: Was the leading cause of diarrhoeal death in Indian children under 5 before the vaccine was introduced.
These are not rare theoretical risks. These diseases circulate in India.
IAP 2025 Vaccination Schedule
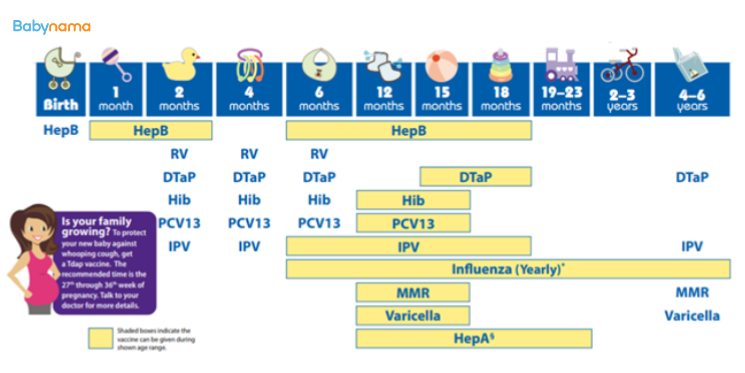
This is the recommended schedule based on the Indian Academy of Pediatrics (IAP) Advisory Committee on Vaccines and Immunization Practices (ACVIP) guidelines, reconciled against India’s Universal Immunization Programme (UIP). “Free (UIP)” means available at government health centres under the Universal Immunization Programme at no cost. “Paid” means available mainly at private clinics. This is the IAP schedule, which differs from the US/CDC schedule — note in particular that the Indian primary series is given at 6, 10 and 14 weeks, not at 2/4/6 months.
One important difference between the IAP and government schedules: UIP provides the Measles-Rubella (MR) vaccine (measles + rubella, no mumps) free at 9 months and 16 months. IAP recommends the MMR vaccine (which also covers mumps); MMR is generally available at private clinics. Where a child receives the free MR doses, a separate mumps-containing MMR may be advised by your pediatrician.
| Age | Vaccine | Free/Paid | Route | Notes |
|---|---|---|---|---|
| Birth | BCG | Free (UIP) | Intradermal | Protects against TB meningitis and miliary TB |
| Birth | Hepatitis B (1st dose) | Free (UIP) | IM | Give within 24 hours of birth |
| Birth | OPV 0 (zero dose) | Free (UIP) | Oral | Birth dose, before discharge |
| 6 weeks | DTwP or DTaP (1st) | Both | IM | DTwP = free govt; DTaP (painless) = paid private |
| 6 weeks | IPV (1st) | Free (UIP) | IM | Injectable polio vaccine |
| 6 weeks | Hepatitis B (2nd) | Free (UIP) | IM | |
| 6 weeks | Hib (1st) | Free (UIP, as Pentavalent) | IM | Combined with DTP+HepB in govt Pentavalent |
| 6 weeks | PCV (1st) | Free (UIP) | IM | Protects against pneumococcal disease |
| 6 weeks | Rotavirus (1st) | Free (UIP) | Oral | Rolled out to all states under UIP; private brands (Rotarix 2-dose, Rotateq 3-dose) also available |
| 10 weeks | DTwP or DTaP (2nd) | Both | IM | |
| 10 weeks | IPV (2nd) | Free (UIP) | IM | |
| 10 weeks | Hib (2nd) | Free (UIP, as Pentavalent) | IM | |
| 10 weeks | PCV (2nd) | Free (UIP) | IM | |
| 10 weeks | Rotavirus (2nd) | Free (UIP) | Oral | |
| 14 weeks | DTwP or DTaP (3rd) | Both | IM | |
| 14 weeks | IPV (3rd) | Free (UIP) | IM | |
| 14 weeks | Hib (3rd) | Free (UIP, as Pentavalent) | IM | |
| 14 weeks | PCV (3rd) | Free (UIP) | IM | |
| 14 weeks | Rotavirus (3rd) | Free (UIP) | Oral | UIP ROTAVAC and Rotateq are 3-dose; private Rotarix is 2-dose (no 14-week dose) |
| 6 months | OPV (1st) | Free (UIP) | Oral | |
| 6 months | Hepatitis B (3rd) | Free (UIP) | IM | Completes primary Hep B series |
| 9 months | MR (1st) under UIP / MMR (1st) IAP | Free (UIP) for MR; MMR paid | SC | UIP gives Measles-Rubella (no mumps); IAP recommends MMR which also covers mumps |
| 9 months | OPV (2nd) | Free (UIP) | Oral | |
| 9–12 months | Typhoid Conjugate (TCV) | Paid | IM | IAP recommends at 9–12 months |
| 12 months | Hepatitis A (1st) | Paid | IM | Two doses 6 months apart |
| 12–15 months | PCV booster | Free (UIP) | IM | IAP times the PCV booster at 12–15 months; under UIP the PCV booster is given around 9 months — confirm local timing |
| 15 months | MMR (2nd) IAP | Paid | SC | IAP 2nd MMR at 15 months; under UIP the 2nd MR dose is given at 16 months (see below) |
| 15 months | Varicella (1st) | Paid | SC | Chickenpox vaccine |
| 15–18 months | DTwP or DTaP booster (1st) | Both | IM | UIP gives DPT booster with the 2nd MR dose around 16–24 months |
| 16 months | MR (2nd) under UIP | Free (UIP) | SC | Government 2nd Measles-Rubella dose, given with the DPT booster |
| 15–18 months | IPV booster | Both | IM | |
| 15–18 months | Hib booster | Paid | IM | Not in UIP booster schedule |
| 18 months | Hepatitis A (2nd) | Paid | IM | |
| 2 years | Typhoid booster | Paid | IM or oral | Oral typhoid vaccine available as alternative |
| 4–6 years | DTwP or DTaP (2nd booster) | Both | IM | |
| 4–6 years | OPV booster | Free (UIP) | Oral | |
| 4–6 years | Varicella (2nd) | Paid | SC | |
| 5 years | MMR (3rd) | Paid | SC | Optional; IAP recommends if 2nd dose given before 15 months |
| 10–12 years | Tdap | Paid | IM | Tetanus, diphtheria, acellular pertussis booster |
| 9–14 years | HPV | Paid | IM | Girls aged 9–14: 2 doses (0 and 6 months). If started at 15 years or older: 3 doses (0, 1–2, 6 months). IAP also notes HPV can be offered to boys |
Note on Pentavalent: The government’s Pentavalent vaccine combines DTP + Hepatitis B + Hib in a single shot. At private clinics, these are often given as separate or as the 6-in-1 (Hexaxim/Infanrix Hexa) which also includes IPV.
Free vs Paid: What You Actually Get Under UIP
The Universal Immunization Programme (UIP)
India’s UIP is one of the largest immunization programmes in the world. All vaccines in the UIP are available free of cost at:
- Government hospitals (district hospitals, sub-district hospitals)
- Community Health Centres (CHCs)
- Primary Health Centres (PHCs)
- Urban Health Centres
- ASHA workers arrange for outreach sessions in villages
Free UIP vaccines (as of 2025):
- BCG (birth)
- Oral Polio Vaccine — OPV (birth, then with later UIP visits; booster at 5 years)
- Hepatitis B (birth, then within the Pentavalent at 6, 10, 14 weeks)
- Pentavalent = DTP + HepB + Hib (6, 10, 14 weeks)
- fIPV / IPV (given at 6 and 14 weeks under UIP)
- PCV (6, 10 weeks and a booster at 9 months) — now rolled out to all states under UIP
- Rotavirus (6, 10, 14 weeks) — now rolled out to all states under UIP
- Measles-Rubella, MR (9 months and 16 months) — note this is MR, not the mumps-containing MMR
- DPT booster (16–24 months and 5–6 years)
- Td (10 years, 16 years)
Note: the exact UIP doses and timing for IPV, PCV and OPV vary slightly by state and have changed over time as the programme expands. Your government health centre or pediatrician will confirm the doses currently offered in your state.
IAP-Recommended Paid Vaccines
These are not “optional extras” — IAP strongly recommends them. They are paid only because they are not yet part of the government programme:
| Vaccine | Approx. Cost per Dose | Disease Prevented |
|---|---|---|
| DTaP (painless) | ₹600–₹900 | Whooping cough, Diphtheria, Tetanus |
| Varicella | ₹1,500–₹2,000 | Chickenpox |
| Hepatitis A | ₹700–₹1,000 | Hepatitis A (jaundice) |
| Typhoid Conjugate (TCV) | ₹700–₹1,200 | Typhoid fever |
| Hib booster | ₹500–₹700 | Hib meningitis (booster) |
| HPV (2-dose series) | ₹2,500–₹3,500 per dose | Cervical cancer |
| MMR 3rd dose (optional) | ₹500–₹800 | Measles, Mumps, Rubella |
Priority if budget is limited: Varicella, Hepatitis A, and TCV provide meaningful additional protection beyond UIP at relatively low cost. HPV is critical for girls approaching adolescence.
Painful vs Painless Vaccines: The DTwP vs DTaP Question
This is the most common vaccine question Indian parents ask. Here is the straight answer.
What They Are
- DTwP (Diphtheria-Tetanus-whole cell Pertussis): Uses a killed whole pertussis (whooping cough) bacterium. More immunogenic. More likely to cause fever and local soreness because the whole-cell component is more inflammatory. This is the vaccine in the government Pentavalent.
- DTaP (Diphtheria-Tetanus-acellular Pertussis): Uses specific purified proteins from the pertussis bacterium rather than the whole cell. Called “painless” because it causes significantly less fever and less local reaction. Available at private clinics as standalone or as part of the 6-in-1 combination vaccine.
IAP’s Position
Both DTwP and DTaP protect against diphtheria, tetanus, and pertussis, and IAP accepts both. Importantly, current IAP ACVIP guidance prefers the whole-cell vaccine (DTwP) for the primary series (the 6-, 10- and 14-week doses), because whole-cell pertussis primes the immune system better and the protection wanes more slowly than with acellular (DTaP). Either can be used for the later boosters. The practical choice is:
- DTwP (Painful): Free at government centres. Slightly stronger immune response. Expect fever within 24–48 hours of each dose, more local redness/swelling at injection site.
- DTaP (Painless): Available at private clinics. Costs ₹600–₹900 per dose (or included in 6-in-1). Fewer side effects. Some studies suggest slightly lower peak antibody levels for pertussis, but clinical protection is comparable.
The honest answer: If the cost difference is manageable for you, DTaP results in a less distressing post-vaccine day. If it’s not, DTwP is not inferior in terms of actual disease protection — your child will be protected. Do not let anyone tell you that choosing DTwP is harmful or that choosing DTaP is unnecessary.
Do not mix DTwP and DTaP within the same primary series (doses 1–2–3) if you can avoid it. Complete the primary series with the same type. Boosters can differ.
Common Side Effects and Management
Vaccine side effects are not complications — they are evidence that your child’s immune system is working. Understanding what is normal prevents unnecessary ER visits and panic.
What to Expect by Age
Birth vaccines (BCG, OPV, Hep B):
- BCG: A small red lump at the injection site (left upper arm) that appears 2–4 weeks after vaccination, ulcerates slightly, and heals leaving a small scar. This is expected and part of a normal vaccine response. Do not squeeze or put anything on it.
- OPV and Hep B at birth: Generally very well tolerated. Mild irritability possible.
6, 10, 14 week vaccines (DTwP/DTaP, IPV, PCV, Rotavirus):
- DTwP: Fever (up to 102°F/38.9°C) within 24 hours, local redness and swelling at injection site, irritability and crying. This is the hardest post-vaccine day in the schedule. It typically peaks at 24–48 hours and resolves by 72 hours.
- DTaP: Much milder. Low-grade fever or no fever, mild local redness. Most children are back to normal within 24 hours.
- PCV: Mild fever, local tenderness. Rarely more.
- Rotavirus: Mild loose stools in some babies. Normal.
9–15 month vaccines (MMR, Varicella):
- MMR: Fever and a mild measles-like rash may appear 7–12 days after vaccination (not immediately). This is expected and not an infection. Child is not contagious. Lasts 2–3 days.
- Varicella: A mild chickenpox-like rash with a few spots can appear 1–3 weeks post-vaccination in up to 5% of children. Very mild. Child may be mildly contagious.
Paracetamol Dosing (Post-Vaccine Fever)
Paracetamol is dosed by your baby’s weight, not age: 15 mg/kg per dose, every 4–6 hours, max 4 doses (60 mg/kg) in 24 hours. Check the syrup strength (120 vs 250 mg/5 ml). Not for under-3-months without a doctor. Confirm the exact mL with your pediatrician.
⚠️ In a baby under 3 months, ANY fever of 100.4°F (38°C) or higher is a medical emergency — see a doctor the same day, even at night. Do not give paracetamol and wait. For the 6-week and 10-week vaccines, do not self-medicate fever; speak to your pediatrician first.
| Child’s Weight | Paracetamol Dose (15 mg/kg) |
|---|---|
| 7 kg (4–6 months) | 105 mg |
| 10 kg (9–12 months) | 150 mg |
| 15 kg (3–4 years) | 225 mg |
Paracetamol syrup (Calpol, Metacin, Febrex) typically comes in 120 mg/5 ml or 250 mg/5 ml concentrations — always calculate and measure the dose based on your child’s weight, not age. Confirm the exact mL with your pediatrician.
Note: Some older guidelines suggested prophylactic paracetamol before the vaccine to prevent fever. Current IAP guidance does not recommend routine prophylactic paracetamol because it may slightly reduce the immune response. Give paracetamol if your child develops fever or significant discomfort, not before.
When to Call Your Doctor
Go back to the clinic or call your pediatrician if:
- Fever is above 104°F (40°C)
- Fever lasts more than 3 days
- The injection site becomes very swollen (more than 5 cm redness), extremely hard, or shows pus
- Your child has inconsolable crying lasting more than 3 hours
- Any rash that spreads significantly or appears to be worsening
🚨 Call 112 (national emergency) or 108 (ambulance), or go to the nearest hospital, if you see: difficulty/noisy breathing; swelling of face/lips/tongue; widespread hives with vomiting; pale/grey/blue skin; floppiness/unresponsiveness; or a seizure. If an adrenaline auto-injector is prescribed, use it first, then go.
Serious allergic reactions (anaphylaxis) are very rare — occurring in roughly 1–2 per million doses. They happen within 15–30 minutes. This is why your clinic keeps you there for observation after vaccination.
Vaccine Myths Debunked
”Vaccines cause autism”
This is the most persistent and most thoroughly disproven myth in modern medicine. Its origin: a 1998 paper by Andrew Wakefield published in The Lancet that claimed a link between the MMR vaccine and autism. What followed was one of the largest fraud investigations in medical history.
Wakefield’s study involved 12 children. He had been paid over £400,000 by lawyers seeking to sue vaccine manufacturers — a conflict of interest he never disclosed. He manipulated the data. The Lancet fully retracted the paper in 2010. Wakefield was struck off the UK medical register (he lost his medical licence). He is not a practicing physician.
Since then, over 20 large-scale studies across millions of children in multiple countries have found zero link between MMR vaccine and autism. The largest — a Danish study of 650,000 children — showed no difference in autism rates between vaccinated and unvaccinated children.
Autism symptoms often become apparent around 12–18 months of age — which coincides with when children receive MMR. This is correlation, not causation. Children who were never vaccinated also develop autism at the same rate.
”Too many vaccines overwhelm the immune system”
A newborn’s immune system can theoretically respond to over 10,000 antigens simultaneously. The total antigens in the entire childhood vaccine schedule are a fraction of what a child’s immune system encounters in a single day of ordinary life. Modern vaccines are highly purified — today’s 14-vaccine schedule contains fewer total antigens than the 1980 schedule of just 4 vaccines. This myth has no scientific basis.
”Natural immunity is better”
In some cases, immunity from surviving a disease is stronger and longer-lasting than vaccine-induced immunity. This is sometimes true. But the price of “natural” immunity from whooping cough is potentially 100 days of violent coughing and possible death in infants. The price of natural measles immunity includes 1-in-1,000 chance of encephalitis. Natural Hib meningitis leaves survivors with permanent hearing loss or brain damage in many cases.
Vaccines train the immune system without paying that price. The argument that “natural is better” ignores that the disease itself is what causes the damage.
”Aluminium in vaccines is dangerous”
Some vaccines contain aluminium salts as adjuvants — they strengthen the immune response. The amount is tiny: about 0.125–0.625 mg per dose. An infant consuming breast milk takes in more aluminium than this. Infants on formula consume significantly more. The aluminium in vaccines is eliminated from the body in weeks. No study has linked vaccine aluminium to harm.
”If my child is healthy and eating well, they don’t need vaccines”
Good nutrition and breastfeeding strengthen immune function but do not provide specific immunity against measles, polio, Hib meningitis, or tetanus. A well-nourished child will get these diseases just as surely as a malnourished one if exposed without vaccination. Nutrition and vaccination are complementary — not alternatives.
”The diseases vaccines prevent don’t exist in India anymore”
Polio was eliminated because of vaccination and would return if we stopped vaccinating — as seen in countries that suspended polio campaigns. Measles cases were reported in Mumbai, Jharkhand, and Rajasthan in 2022–23. Whooping cough cases are reported every year. Typhoid is extremely common in India. These diseases exist. Vaccination is why we don’t see the mortality numbers of 30 years ago.
Missed Vaccines and Catch-Up Schedule
The Core Principle: It Is Never Too Late
If your child has missed vaccines — for any reason — do not assume the opportunity has passed. IAP has a catch-up schedule. Children who have never been vaccinated can start at any age. Children who started but fell behind can resume without restarting.
Key Catch-Up Rules
- Never restart a series. If your child received 2 doses of DTaP and then you missed the 3rd, give the 3rd and continue from there. You do not start over.
- Minimum intervals apply. There are minimum intervals between doses for each vaccine to ensure proper immune response. Your pediatrician will calculate these.
- Maximum age limits for some vaccines. Rotavirus cannot be started after 15 weeks (1st dose limit) and cannot be given after 8 months of age — the last dose must be completed by 8 months 0 days (IAP/ACVIP). This is a hard cutoff.
- No maximum age for most vaccines. BCG can be given up to 5 years in unvaccinated children. MMR has no upper age limit. Hepatitis B can be given to adults.
- HPV works best when given to girls aged 9–14 (2-dose schedule) before sexual debut; it can still be given to older adolescents and young adults (3-dose schedule). Discuss timing with your pediatrician.
Common Catch-Up Scenarios
Child is 6 months old and has received no vaccines:
- Give BCG, OPV, DTaP/DTwP, IPV, PCV, Hep B at the first visit. Do not give Rotavirus (past age limit for starting if beyond 15 weeks). Then space remaining doses per minimum intervals.
Child is 3 years old and only got birth vaccines:
- Give MMR (1st), Varicella, Hep A (1st), TCV, DTwP/DTaP immediately. Schedule remaining doses. Rotavirus cannot be given at this age.
Child missed the 15–18 month DTP booster:
- Give it now, regardless of how late. Then schedule the 4–6 year booster.
Always bring whatever vaccination records you have (the Immunization Card from the government centre, or the private clinic’s vaccination booklet). Your pediatrician will determine what is needed.
Government Centres vs Private Clinics
At Government Hospitals and PHCs
What you get: All UIP vaccines — free. BCG, OPV, Hep B, Pentavalent (DTwP+HepB+Hib), IPV, PCV, Rotavirus (in select states), MMR, DTP booster, Td.
What to bring: Your child’s previous vaccination card. If it’s the first visit, they will issue one.
Practical notes:
- Immunization sessions at PHCs are typically held on fixed days (often Tuesday and Friday). Check your local PHC schedule.
- Urban Health Centres and district hospitals often have daily immunization.
- ASHA workers in your area can tell you the nearest session and help with scheduling.
- Cold chain is maintained under the government’s cold chain network — vaccines are kept at 2–8°C throughout. Do not accept vaccines from a centre where you see the fridge door left open or the power supply is inconsistent.
At Private Clinics
What you get: All UIP vaccines plus all IAP-recommended paid vaccines. More flexibility in scheduling. Can choose DTaP over DTwP.
What to check:
- Ask your pediatrician how vaccines are stored. A good clinic stores vaccines in a dedicated vaccine refrigerator, not a food fridge. Vaccines should never be in the door compartment (temperature fluctuates too much there).
- Ask for the vaccine name, batch number, and manufacturing date before injection. You can refuse if a vial looks cloudy when it should be clear, or if the VVM (Vaccine Vial Monitor) square on the vial is dark.
Cold chain is critical. A vaccine kept too warm is not just less effective — it may appear effective while providing no real protection. Both government and private cold chain systems in India have been audited and improved significantly since 2015, but spot-checking what you can is always reasonable.
Vaccines in Special Situations
Premature Babies
Vaccinate on actual (chronological) age, not corrected gestational age — with one exception. BCG should wait until the baby weighs at least 2 kg.
A 28-week preterm baby born in January should receive their 6-week vaccines at 6 weeks of actual life (March), even though their corrected age is still around 35–36 weeks gestation. The immune response in preterm infants is slightly lower but still clinically protective. Premature babies are more vulnerable to infections like pertussis and RSV — vaccinating on time is especially important.
Hepatitis B for very low birth weight babies (under 2 kg): the birth dose may be less immunogenic. An additional dose is given, making it a 4-dose series for these babies.
Immunocompromised Children
Children on immunosuppressive therapy (chemotherapy, high-dose steroids, post-organ transplant) need specialist guidance:
- Live vaccines (MMR, Varicella, OPV, live typhoid oral) are generally contraindicated in significantly immunocompromised children.
- Inactivated vaccines (IPV, IPV, DTaP, Hep B, Hep A, TCV, PCV, flu shot) are generally safe but may produce a weaker immune response.
- If immunosuppression is planned (for example, before chemotherapy), try to complete all age-appropriate vaccines at least 2 weeks before starting treatment.
- After transplant or chemotherapy, the vaccination schedule often needs to be restarted — consult your child’s hematologist/oncologist alongside the pediatrician.
Child Has a Fever or Illness Today
Mild illness (cold, mild cough, low fever under 38°C, mild diarrhoea) is not a reason to postpone vaccines. Delay is often more harmful than administering the vaccine to a mildly ill child.
Postpone if your child has:
- High fever (over 38.5°C / 101.3°F) — wait until it resolves
- A severe, acute illness — wait until better
- A moderate or severe diarrhoeal illness — postpone oral vaccines (OPV, Rotavirus) only; injectable vaccines can proceed
Egg Allergy and MMR
The old recommendation to avoid MMR in egg-allergic children is outdated. MMR is not grown in eggs. It is grown in chick embryo fibroblast culture, which contains negligible egg protein. Major allergy bodies, including the American Academy of Allergy, Asthma & Immunology, and IAP, confirm that egg allergy is not a contraindication to MMR.
Children with egg allergy, including those with anaphylactic egg allergy, can safely receive MMR in a standard clinical setting. No special precautions beyond the routine 15-minute post-vaccine observation are needed.
Influenza vaccines can be grown in eggs and may contain egg proteins — that is where egg allergy is genuinely relevant. Even for flu vaccines, egg-free formulations are increasingly available.
Travel Vaccines
Travelling Within India
India’s disease landscape is non-uniform. Travelling from a low-burden urban area to regions with different sanitation, water quality, or disease burden increases risk.
Hepatitis A: Transmitted through contaminated food and water. India has high endemicity. If your child is unvaccinated and you are travelling to areas with questionable water/sanitation (which includes most of rural India), Hepatitis A vaccine is strongly advisable. Two doses provide long-lasting protection.
Typhoid: Typhoid fever is endemic across India and particularly common in areas with inadequate sanitation. TCV (Typhoid Conjugate Vaccine) from 6 months of age is an IAP recommendation, not just a travel vaccine — but if your child is unvaccinated and travelling to high-risk areas, prioritise this.
Japanese Encephalitis (JE): JE vaccine is part of the UIP in endemic areas (northeastern India, parts of UP, Bihar, Karnataka, West Bengal). If travelling to these areas from a state where JE vaccine was not given, consider it.
International Travel
For international travel, requirements depend on destination. Key considerations:
- Yellow Fever: Required for entry into many African and South American countries. Mandatory if travelling from a yellow fever endemic country. Certificate required. Child must be at least 9 months old.
- Meningococcal vaccine: Required for Hajj/Umrah (Saudi Arabia requires ACWY vaccination).
- Influenza: Not part of the standard IAP schedule but recommended for travel, especially to countries with active flu circulation.
- COVID-19 vaccines: Requirements vary by country and continue to change.
- Hepatitis A and Typhoid: Already recommended for all Indian children, but prioritise if unvaccinated before travel.
Consult a travel medicine clinic at least 4–6 weeks before international travel, as some vaccines require multiple doses or specific timing.
Vaccines in the Pipeline for India
Dengue Vaccine
A dengue vaccine (Dengvaxia, by Sanofi) is approved in some countries but has a critical limitation: it should only be given to people who have already been infected with dengue at least once. Giving it to dengue-naive individuals can increase the risk of severe dengue on subsequent infection. India has not approved Dengvaxia for public use. A newer dengue vaccine (TAK-003 by Takeda) has shown better results without the seropositive-only restriction and is under regulatory review in several countries. Not yet available in India as of early 2026.
Malaria Vaccine (RTS,S / R21)
The RTS,S vaccine (Mosquirix) and R21/Matrix-M vaccine (Oxford/Serum Institute) represent the first approved malaria vaccines. WHO recommended RTS,S in 2021 and R21 in 2023. R21 is manufactured by Serum Institute of India. Clinical trials and initial rollouts are ongoing in sub-Saharan Africa, where malaria burden is highest. India has not yet introduced routine malaria vaccination, but given Serum Institute’s manufacturing role and India’s malaria burden, this is a realistic near-term development.
RSV Vaccine
Respiratory Syncytial Virus (RSV) causes serious lower respiratory infections in infants. Nirsevimab (Beyfortus), a long-acting monoclonal antibody, has been approved in the US and Europe to protect infants through RSV season. This is not a traditional vaccine but functions similarly. Maternal RSV vaccines (given to pregnant women to pass immunity to the newborn) are also approved in some countries. These are not yet available in India but are expected to be introduced in the coming years.
Newer Typhoid Vaccines
Typbar-TCV by Bharat Biotech (made in India) is the world’s first WHO-prequalified typhoid conjugate vaccine and is already used in India. Nepal, Pakistan, and Zimbabwe have introduced it into national programmes. India’s government is evaluating UIP inclusion.
Frequently Asked Questions
My baby cried a lot after the 6-week vaccines. Is this normal?
Yes. The 6-week DTwP shot (the painful DTP variant given at government centres) causes significant local discomfort and often fever. Inconsolable crying in the first few hours is common and is not a reason to panic. Offer extra feeds and provide skin-to-skin contact. For fever or significant discomfort, paracetamol is dosed by weight (15 mg/kg), but in a baby under 3 months do not give paracetamol on your own — speak to your pediatrician first, and remember that in an under-3-month-old any fever of 100.4°F (38°C) or higher is a same-day emergency. If crying persists beyond 3 hours, or the child becomes limp/unresponsive or has difficulty breathing, call 112 or 108 or go to the nearest hospital.
Can I give two vaccines on the same day?
Yes. Multiple vaccines given at the same visit are safe and effective. The immune system handles multiple antigens simultaneously without difficulty. Combination vaccines (like Pentavalent or the 6-in-1) exist precisely to reduce the number of injections while maintaining coverage. IAP’s entire schedule is designed around same-day administration.
My child had a high fever after a vaccine. Will it happen again with the next dose?
Fever after DTwP does not predict fever with certainty after subsequent doses — the reaction can vary. However, if your child had a very high fever (over 40°C) or an unusual reaction after a previous dose, discuss switching from DTwP to DTaP for remaining doses with your pediatrician. This is a recognised option.
My 5-year-old has never been vaccinated. Can we start now?
Yes. Start immediately. Some vaccines can no longer be given past certain ages (Rotavirus), but most of the important vaccines — DTaP, IPV, MMR, Varicella, Hep A, Hep B, TCV, PCV — have no upper age limit or an upper limit that a 5-year-old falls well within. Your pediatrician will draw up a catch-up schedule.
Is there a vaccine that prevents all fevers?
No. Vaccines prevent specific diseases caused by specific pathogens. They do not prevent fever from other viruses (there are hundreds that circulate in India), bacterial infections not covered by vaccines, or non-infectious causes of fever. A vaccinated child will still get colds and fever — just not the specific diseases the vaccines target.
The government BCG leaves a scar. Is that a problem?
The BCG scar is expected and indicates a successful vaccine response. It is not a problem. In India, the BCG is given intradermally on the left upper arm and results in a small pustule that ulcerates and heals over several weeks, leaving a 4–8 mm scar. An absent BCG scar may indicate a failed vaccination — discuss with your pediatrician whether a repeat dose is needed (before 5 years of age).
Can I space out the vaccines instead of following the schedule?
IAP and the WHO do not recommend spreading out or delaying vaccines without medical cause. Spacing out vaccines means your child is unprotected against multiple serious diseases for longer. It does not reduce side effects meaningfully (since each vaccine is typically given at its own visit in the spaced-out approach, you are just multiplying the number of doctor visits and unprotected windows). The schedule is designed to provide protection as early as possible while the immune system can mount an adequate response. Follow the schedule.
This guide reflects IAP 2025 guidelines and is reviewed by Babynama pediatricians. It is for informational purposes and does not replace advice from your child’s doctor. For individual medical decisions, consult your pediatrician.
Real Questions from Indian Mothers
These are real questions asked by parents in the Babynama community, answered by our pediatricians.
“My baby is 1.5 months old and since when he has got his vaccination he is kinda reckless, doesn’t relax like before vaccination. Mostly cranky and crying. He had colic issue 3-4 days but now he is better but still cranky. What could be the reason?”
This can happen post vaccination. Apply an ice pack wrapped in cloth at the vaccination site and distract the baby. In a baby this young (under 3 months), do not give paracetamol on your own — and any fever of 100.4°F (38°C) or higher is a same-day emergency, so see your pediatrician the same day rather than treating fever at home. For pain that does not settle, check with your pediatrician about the correct weight-based dose.
“Good afternoon mam,today my got dpt vaccine she is crying a lot and had swelling a lot and feeding only on non injected side of leg mam,please give me suggestion and help me out”
Yes Post vaccination take care in the way as — • injection site if red and hardened- apply ice wrapped in cotton cloth • if fever (more than or equal to 100F) give paracetamol drops
“Do vaccination cause diarrhoea in babies?”
Post vaccination there can be change in sleep pattern, stool pattern, feeding and fever might also occur. If baby is active & feeding well, observe for now and breastfeed every 2-3 hourly to maintain baby’s hydration
“Does these vaccines are available in painless? Which one you suggest painless or normal?”
Yes Effectivity of both vaccines is same However painless vaccine cause less side effects like less pain less irritability less fever less redness. Ultimately it’s parents choice